Introduction
The physical environment of a healthcare facility is an active factor in patient and staff safety. A blocked corridor during a fire evacuation, an unlabeled utility shutoff during an emergency, or a pharmacy with inadequate access control can each produce serious consequences. The Joint Commission's Environment of Care (EC) standards convert that responsibility into auditable, enforceable requirements.
Those requirements carry weight well beyond the accreditation survey. For security professionals and facility managers, the EC framework provides a documented structure for managing risks that otherwise build undetected across hospitals, ambulatory care centers, behavioral health facilities, and nursing care centers — until an incident makes them visible. Compliance reduces liability, protects occupants, and keeps operations functional when conditions deteriorate.
This guide covers what the EC standards require, how the management plans work in practice, what surveyors actually scrutinize, and how to avoid the compliance gaps that trip up even well-resourced organizations.
TL;DR: Key Takeaways
- The EC standards govern how accredited organizations manage physical hazards — covering safety, security, hazardous materials, fire safety, medical equipment, and utility systems
- As of January 1, 2026, hospitals and critical access hospitals operate under a consolidated "Physical Environment" (PE) chapter; non-hospital settings retain the EC chapter designation
- All six required management plan areas must be documented and evaluated annually
- Security management is among the most frequently updated and surveyor-scrutinized EC components, with workplace violence prevention drawing particular attention
- Staff interview readiness is a critical and commonly underestimated gap during surveys
What Are the Joint Commission Environment of Care Standards?
The EC standards define how accredited organizations must manage the physical environment to keep patients, visitors, and staff safe. The framework covers everything from equipment maintenance and hazardous waste handling to building security and fire evacuation — and it requires ongoing management, not just policy documents sitting in a binder.
Who Must Comply
Compliance obligations vary by setting:
- Hospitals and critical access hospitals — now governed by the new Physical Environment (PE) chapter effective January 1, 2026
- Ambulatory care, behavioral health, and nursing care centers — continue operating under the original EC chapter structure
- Laboratories and other accredited settings — subject to applicable EC requirements based on their accreditation program
The Accreditation 360 Restructuring
For hospitals and critical access hospitals, the Joint Commission's Accreditation 360 initiative consolidated the former EC and Life Safety (LS) chapters into a single "Physical Environment" chapter, effective January 1, 2026. According to the Joint Commission, this restructuring removed 714 requirements from the hospital accreditation program and 649 from the critical access hospital program.
The Joint Commission's PE webinar materials state that "no new concepts have been introduced" — the core substance of requirements remains intact. Standards and elements of performance were renumbered and reorganized, not eliminated in substance.
The restructuring also more clearly aligns PE requirements with CMS Conditions of Participation.
For non-hospital settings, the Accreditation 360 changes do not apply — the Environment of Care chapter designation and structure continue unchanged.
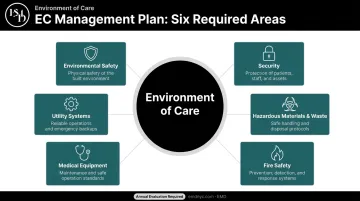
The Six EC Management Plans: A Complete Breakdown
The Joint Commission FAQ confirms six required EC management plan areas: environmental safety, security, hazardous materials and waste, fire safety, medical equipment, and utility systems. Separate documents aren't required — organizations may combine areas into one plan — but each area must be addressed, customized to the facility's specific context, and evaluated annually.
Safety and Security Management
Safety management addresses broad hazard identification and mitigation — slips, trips, falls, unsecured equipment, unsafe storage. It requires:
- Designation of a responsible individual (e.g., a safety officer)
- Formal environmental tours at six-month intervals in patient care areas, twelve-month intervals elsewhere
Security management covers a wider risk surface:
- Unauthorized access prevention
- Workplace violence prevention programs, evaluated annually using incident data and staff feedback
- Infant and pediatric abduction prevention
- Protection of security-sensitive areas: pharmacy, obstetrics, server rooms
Surveyors evaluate whether workplace violence programs are data-driven — not just documented, but informed by real incident history and staff input.
Hazardous Materials and Waste Management
This plan covers chemicals, chemotherapeutic agents, radioactive materials, and infectious waste. Key requirements:
- Current inventory with accessible Safety Data Sheets (SDSs) compliant with OSHA's Globally Harmonized System
- Staff training when new chemicals are introduced
- OSHA 29 CFR 1910.1200(g)(8) requires SDSs to be accessible during every work shift — electronic systems must include a downtime contingency
- Paper backup or offline access is required when primary systems are unavailable
Surveyors ask directly whether staff can access SDSs if the server goes down. Organizations without a paper backup or offline system are exposed.
Fire Safety and Life Safety Management
Healthcare facilities use a "defend in place" strategy: rather than evacuating the full building, patients are moved horizontally within smoke compartments. This approach shapes fire drill design and staff training at every level.
Critical requirements:
- All staff, including EVS and contract personnel, must understand RACE/PASS protocols
- Staff should be able to identify smoke compartment boundaries
- Fire drills must be conducted once per shift per quarter, with audible and visual alarms activated
- Per Joint Commission Resources guidance, contract workers and licensed independent practitioners fall within staff responsibilities under the fire response plan
Medical Equipment and Utility Systems Management
Medical equipment requirements include a complete inventory, preventive maintenance schedules, and removal from service of equipment with outstanding safety concerns.
Utility systems management covers HVAC, medical gas, emergency power, and water management. Key points:
- Utility system controls must be labeled for partial or complete emergency shutdown (EC.02.05.01 EP 9)
- Ventilation systems in operating rooms, isolation rooms, and critical care areas must maintain specific pressure relationships, air-exchange rates, filtration efficiencies, temperature, and humidity — per NFPA 99-2012 and ASHRAE 170
- All systems must be regularly tested with documented results
EC Documentation and Committee Requirements
What Surveyors Expect to See
Documentation gaps are one of the most common reasons organizations receive findings. Surveyors look for:
- Current management plans with documented annual evaluations
- Meeting minutes showing attendance, action items, accountability assignments, and due dates
- Maintenance records for fire systems and utility infrastructure
- Fire drill records, including participation rates for contract staff and licensed independent practitioners
- Environmental tour findings with resolution timelines
Annual evaluations must be substantive. Specifically, each evaluation should:
- Confirm whether prior-year objectives were achieved
- Identify new hazards or program changes since the last cycle
- Set improvement objectives for the coming year
Committee Structure
The Joint Commission does not mandate a formal EC or safety committee. Instead, it requires designated individuals to manage risk, coordinate risk-reduction activities, collect deficiency data, and report summaries to leadership. In practice, most organizations use a multidisciplinary committee.
One threshold matters: if a responsible group meets less frequently than quarterly, surveyors will likely require a satisfactory explanation of how it effectively manages the dynamic conditions of a healthcare organization.
How that committee performs — and how well it documents its work — directly affects how survey findings are scored.
The SAFER Matrix
Survey findings are plotted on the SAFER (Survey Analysis for Evaluating Risk) Matrix across two dimensions:
| Axis | Categories |
|---|---|
| Likelihood of harm | Low / Moderate / High |
| Scope | Limited / Pattern / Widespread |
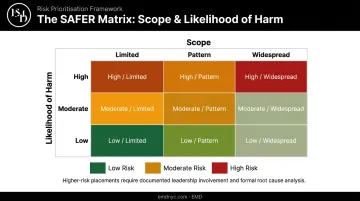
Higher-risk findings require more detailed corrective action responses, including evidence of leadership involvement and root cause analysis. Organizations with organized, current documentation can respond to these findings faster and with greater credibility — leadership can point to specific records rather than reconstructing history under pressure.
Building a Compliant Security Management Plan
Security is among the most frequently updated and surveyor-scrutinized areas of EC compliance. A compliant security management plan must demonstrate:
- A documented, current risk assessment process
- Defined access control roles for sensitive areas (pharmacy, pediatrics, server rooms)
- A workplace violence prevention program informed by staff incident data
- Protocols for responding to security events, tailored to the specific facility type
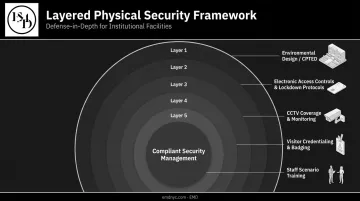
The Layered Security Approach
Effective security management isn't a single system — it's overlapping layers:
- Electronic access controls, mantraps, and after-hours lockdown protocols at every entry point
- CCTV coverage mapped directly to risk-identified areas, not installed by default
- Visitor credentialing and badging with documented flow management procedures
- Staff training built around scenario exercises, not just annual classroom attendance
- Environmental design using CPTED principles at entry points, parking areas, and wayfinding routes
Organizations frequently underestimate how rigorously surveyors scrutinize documentation. Risk assessments must be current, site-specific, and tied directly to corrective actions — generic security awareness statements will not satisfy a Joint Commission reviewer.
Where a Security Consulting Partner Adds Value
EMD, a physical security consulting firm with experience across hospitals, behavioral health facilities, ambulatory surgery centers, and emergency departments, uses AI-augmented vulnerability assessments paired with on-site human analysis to evaluate healthcare environments against real-world threat scenarios. Their consulting scope addresses ED access, behavioral health unit safety, infant and pediatric protection, medication storage, and workplace violence prevention — all areas where Joint Commission surveyors look closely.
These same assessment principles extend beyond healthcare settings. Schools, campuses, museums, and houses of worship face incident-driven security vulnerabilities that mirror those cited in healthcare surveys. Each benefits from the same structured approach: documented risk assessment, layered access controls, and staff preparedness built around actual incident data.
Common Survey Findings and How to Avoid Them
Most-Cited Deficiency Categories
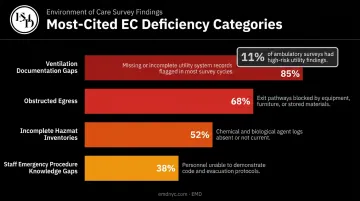
Based on Joint Commission publication materials, recurring EC survey findings cluster in several areas:
- Ventilation documentation gaps — missing or incomplete records for operating rooms, isolation rooms, and critical care areas
- Obstructed egress — corridors and exits blocked by equipment or storage
- Incomplete hazardous materials inventories — outdated SDSs or inaccessible records
- Staff who can't articulate emergency procedures — particularly EVS, maintenance, and security staff
Ventilation documentation deserves particular attention. Joint Commission survey data for ambulatory settings found that 11% of surveys had high-risk findings related to inspection, testing, and maintenance of utility equipment — with ventilation parameters, OR positive pressure, and air exchange rates among the most common issues. Manual monitoring processes are especially prone to gaps during nights, weekends, and shift changes — making consistent documentation discipline a key exposure point for facilities relying solely on paper-based tracking.
The Internal Policy Trap
Organizations that write internal policies exceeding Joint Commission requirements are still cited when they fail to meet their own more stringent benchmarks. Aligning internal policy language as closely as possible with actual regulatory requirements eliminates this self-imposed exposure.
Proactive Preparation Strategies
Tightening policy language is one piece of the puzzle. Sustained operational readiness requires a broader preparation approach:
- Conduct regular mock surveys with deficiency-on-the-spot resolution
- Integrate EC awareness into daily huddles, not just annual training
- Ensure leadership actively participates in environmental rounds
- Validate staff knowledge through brief scenario-based exercises — not just classroom instruction
Staff interview readiness is consistently underestimated. Surveyors routinely ask frontline workers — EVS, maintenance, security personnel — about their specific roles during fire events, utility failures, and medical emergencies. Facilities that embed scenario-based Q&A into regular training cycles give staff the language and confidence to respond accurately when it counts.
Frequently Asked Questions
What are the Joint Commission Environment of Care standards?
The EC standards are Joint Commission accreditation requirements governing how healthcare organizations manage physical hazards across six areas: safety, security, hazardous materials, fire safety, medical equipment, and utility systems. Compliance requires documented management plans, ongoing risk assessments, and continuous performance monitoring to protect patients, staff, and visitors.
What are the six Joint Commission EC management plan areas?
The Joint Commission FAQ confirms six required management plan areas: environmental safety, security, hazardous materials and waste, fire safety, medical equipment, and utility systems. Emergency management is addressed separately. Each area requires documentation, risk assessments, and annual evaluations, and all six areas can be combined into a single document.
What is the difference between the EC chapter and the new Physical Environment chapter?
As of January 1, 2026, the Joint Commission merged its EC and Life Safety chapters into a single "Physical Environment" chapter for hospitals and critical access hospitals under Accreditation 360. Non-hospital settings, including ambulatory care, behavioral health, and nursing care centers, continue under the original EC chapter designation.
How often must EC management plans be reviewed?
Joint Commission requires each management plan to be evaluated at least annually to assess effectiveness, reflect operational changes, and identify improvement opportunities. Joint Commission expects ongoing monitoring and committee review throughout the year; the annual evaluation is a formal checkpoint within a continuous process.
What happens if a survey finds EC deficiencies?
Findings are plotted on the SAFER Matrix by likelihood of harm and scope. Higher-risk findings require corrective action plans with leadership involvement and root cause analysis, demonstrated through Evidence of Standards Compliance — failure to show progress can trigger follow-up surveys or affect accreditation status.
What is the SAFER Matrix?
The SAFER Matrix plots each survey finding by likelihood of harm (low, moderate, or high) and scope (limited, pattern, or widespread). Higher-risk placements on the matrix require documented leadership involvement and preventive analysis, with more corrective action detail than lower-risk findings.