According to the Bureau of Labor Statistics, healthcare and social assistance accounted for 72.8% of all private-industry workplace violence cases in 2021–2022. The American Hospital Association estimates the total annual financial cost of violence to U.S. hospitals at $18.27 billion — a figure that reflects not just security failures, but the organizational cost of not acting proactively.
A physical security vulnerability assessment is a structured, expert-led process to identify, prioritize, and document security weaknesses before they become incidents. It's not a building walkthrough or a compliance checkbox — it's a systematic evaluation of every layer of physical risk, from perimeter access to staff safety protocols.
This guide covers who needs these services, what the assessment process looks like, how it maps to regulatory requirements, and what to look for when choosing a provider.
Key Takeaways
- Healthcare facilities face disproportionate workplace violence risk — and physical security gaps are frequently the root cause
- Vulnerability assessments go beyond a single walkthrough — covering access control, surveillance, ED entry points, behavioral health units, and infant protection
- The Joint Commission and CMS Conditions of Participation require documented, recurring security risk analysis
- Risk-based prioritization matters: not every gap can be addressed immediately in a 24/7 clinical environment
- The right provider understands clinical workflows, regulatory requirements, and healthcare's distinct threat environment
Why Healthcare Facilities Are Prime Physical Security Targets
Healthcare environments carry a combination of factors that make them uniquely difficult to secure.
Patients and visitors are often in acute distress. Emergency departments operate around the clock with open access policies. Behavioral health units concentrate high-risk interactions. And unlike most workplaces, healthcare facilities cannot restrict access in the way a corporate office or school might — care has to keep moving.
The data reflects this exposure:
- Type 2 workplace violence — patients or visitors attacking staff — accounts for 84.2% of aggravated assaults and 89.5% of simple assaults in hospitals, per the IAHSS Foundation's 2025 Healthcare Crime Survey
- Healthcare workers are 4 to 5 times more likely to suffer workplace violence injuries than workers in other industries, according to The Joint Commission
- In 2020, 76% of all private-industry workers who experienced trauma from nonfatal workplace violence worked in healthcare and social assistance

The physical environment compounds this exposure. Structural vulnerabilities common across healthcare settings include:
- Aging facilities with outdated or absent access control systems
- Multi-building campuses with numerous entry points that are difficult to monitor
- After-hours access gaps that daytime staffing and activity levels tend to mask
- Parking structures, loading docks, and service corridors that fall outside primary security coverage
These vulnerabilities carry direct regulatory weight. CMS Conditions of Participation (42 CFR 482.13, 482.41) require hospitals to maintain patient safety and a secure physical environment. The Joint Commission's Standard EC.02.01.01 mandates annual worksite analysis for workplace violence prevention and documented mitigation of identified risks.
The financial stakes reinforce the case for proactive assessment. Incident response costs — staff injury claims, investigations, legal exposure, and operational disruption — routinely exceed what a structured vulnerability assessment would have cost upfront.
What Does a Healthcare Physical Security Vulnerability Assessment Cover?
A professional physical security vulnerability assessment covers more than doors and cameras. It examines every layer of the physical environment where threats can enter, escalate, or go undetected.
Perimeter, Entry, and Access Control
The assessment evaluates how the facility controls who enters and where they can go. This includes:
- Perimeter fencing, vehicle barriers, and parking lot lighting
- Entry screening processes and staffing at primary access points
- After-hours access controls for staff and contractors
- Electronic access systems, key card management, and credentialing gaps
- Emergency department and behavioral health unit entry — both high-risk zones with distinct access challenges
Unmonitored entry points, propped doors, tailgating risks, and inadequate visitor credentialing are among the most common findings in healthcare access control assessments.
Surveillance and Intrusion Detection
The assessment reviews CCTV coverage across the facility, evaluating:
- Blind spots and camera placement relative to high-risk areas
- Whether monitoring is active or passive
- Staff capacity to respond in real time to camera feeds
- Intrusion detection systems and duress/panic alarm coverage
- Emergency notification systems for after-hours zones and isolated work areas
The Joint Commission is clear: remote camera monitoring alone does not constitute "constant surveillance" unless staff can immediately react to minimize risk. That distinction matters when documenting compliance gaps.
Clinical-Area-Specific Security
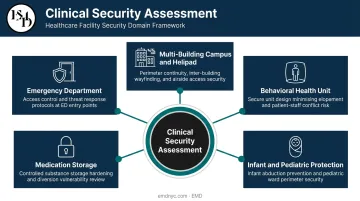
Healthcare facilities carry a specialized risk profile that general commercial assessments don't address. A healthcare-focused assessment covers:
- Emergency department access and waiting-room security — including weapon screening, sightline design, and staff escape routes
- Behavioral health unit safety — environmental design that reduces patient and bystander violence risk
- Infant and pediatric protection — evaluating controls against offender impersonation and unauthorized removal
- Medication storage security — compliance with 21 CFR Part 1301 physical controls for controlled substances and CMS 42 CFR 482.25 requirements
- Multi-building campus access and helipad security
Operational and Human-Factor Risks
Security hardware only works when the people using it know what to do. Operational factors reviewed include:
- Visitor management policies and credentialing procedures
- Lockdown and run-hide-fight protocols
- Staff training currency and drill frequency
A facility can have adequate cameras and still lack any clear protocol for what staff should do when something is observed. That gap — between equipment and action — is where assessments most often surface critical findings.
The Physical Security Assessment Process: What Healthcare Organizations Can Expect
Step 1 — Scoping and Site Discovery
The engagement starts by defining what's in scope: buildings, entry points, clinical units, off-site locations, and campus infrastructure. For healthcare organizations, scope typically extends beyond the main building to include emergency department access, behavioral health wings, parking structures, and loading docks.
Any location where patients or staff could be at risk is part of that picture.
Asset discovery often surfaces gaps — entry points that aren't documented in facility maps, camera systems that haven't been reviewed in years, or areas where access control records don't match physical reality.
Step 2 — Physical Vulnerability Identification
Assessors conduct on-site evaluation of physical infrastructure and operational processes. EMD's AI-augmented methodology goes beyond a standard walkthrough by modeling how vulnerabilities intersect across systems — analyzing, for example, how a gap in after-hours access control intersects with insufficient surveillance coverage in a specific zone. This layered analysis identifies risk scenarios that individual system reviews miss.
Assessment areas typically include:
- Perimeter and entry point security
- CCTV coverage and active monitoring capability
- Access control and credentialing processes
- Visitor management and identification protocols
- Duress alarm and emergency notification systems
- Lighting, sightlines, and environmental design
Step 3 — Risk-Based Prioritization
Not every finding carries the same urgency. A gap in visitor credentialing at an emergency department entrance ranks differently than a lighting deficiency in an administrative parking lot. Findings are prioritized based on three factors:
- Threat likelihood — how probable is exploitation given current conditions
- Potential consequence — impact on patients, staff, or operations if the gap is exploited
- Area vulnerability — sensitivity of the affected space (clinical vs. administrative)
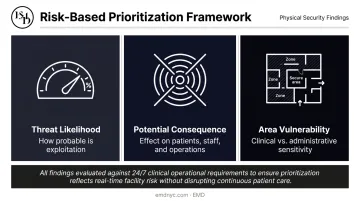
For clinical environments, prioritization accounts for the 24/7 operational reality — some improvements can be implemented immediately, while others require phased planning that doesn't disrupt patient care.
Step 4 — Reporting and Remediation Guidance
The final report organizes findings by severity and affected area, with specific remediation recommendations for each. For healthcare clients, EMD's reports are structured to serve both facility security directors and compliance stakeholders, with findings that map to The Joint Commission environment-of-care standards and CMS Conditions of Participation.
The report goes further than identifying problems. Remediation guidance translates findings into a practical implementation roadmap, and where applicable, identifies federal or state grant funding that may offset improvement costs.
Step 5 — Post-Assessment Support and Design
After the assessment, the work continues. EMD provides follow-on security design consulting that addresses identified gaps through specific physical security improvements: access control upgrades, CCTV redesign, perimeter hardening, behavioral health unit redesign, and more.
For eligible 501(c)(3) nonprofit healthcare organizations, this includes support for Nonprofit Security Grant Program (NSGP) applications. The NSGP funds physical security target-hardening including access control, surveillance, perimeter security, and ballistic glazing.
Compliance Requirements for Healthcare Physical Security Assessments
Joint Commission Environment-of-Care Standards
The Joint Commission's workplace violence prevention standards, effective for hospitals in 2022, include direct physical security requirements:
- EC.02.01.01 EP 17: Annual worksite analysis related to workplace violence prevention and mitigation of identified risks
- LD.03.01.01 EP 9: A workplace violence prevention program led by a designated individual and developed by a multidisciplinary team
- EC.04.01.01: Monitoring and investigation of security incidents involving patients or staff
- HR.01.05.03 EP 29: Education and training at hire and annually
These standards require documented, recurring assessments.
CMS Conditions of Participation
CMS imposes several overlapping physical security obligations on hospitals:
- Protect patients in a safe setting and maintain the physical environment for patient safety (42 CFR 482.13, 482.41)
- Maintain an all-hazards emergency preparedness program based on risk assessment (42 CFR 482.15)
- Keep all drugs and biologicals in secure areas, with Schedule II–V controlled substances locked (42 CFR 482.25)
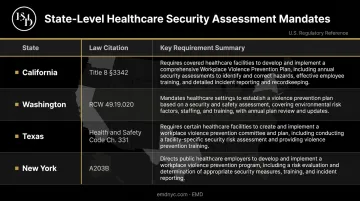
State Workplace Violence Prevention Laws
Several states have enacted binding requirements beyond federal guidance:
| State | Key Requirement |
|---|---|
| California | Title 8 §3342 — mandatory violence prevention plan with engineering controls |
| Washington | RCW 49.19.020 — annual plan review and update (effective January 2026) |
| Texas | Health & Safety Code Ch. 331 — prevention committee and written plan |
| New York | A203B — violence prevention program with security assessment requirements |
A physical security vulnerability assessment generates the documented evidence these frameworks require: worksite analysis records, identified risks, mitigation decisions, and proof of corrective actions.
How to Choose the Right Physical Security Assessment Provider
Clinical environments carry risk profiles, regulatory obligations, and operational constraints that most general security consultants aren't equipped to address. Choosing the right provider means verifying real healthcare expertise — not just broad security experience.
Evaluate any prospective provider against these criteria:
- Healthcare-specific experience: Confirm direct work with emergency departments, behavioral health units, infant security protocols, and multi-building campus design. Ask whether they understand Joint Commission environment-of-care standards and CMS Conditions of Participation — not just general security best practices.
- Methodology depth: A credible assessment combines on-site physical evaluation with operational process review and analysis that models how vulnerabilities interact across systems. Providers who rely solely on a walkthrough checklist miss the layered risk picture clinical environments require.
- Actionable deliverables: The report should serve both security operations staff and compliance stakeholders. Ask whether the provider can translate findings into security design solutions and support grant funding applications if your organization qualifies.
If you're ready to move from evaluation criteria to an actual assessment, EMD works with hospitals, urgent care centers, behavioral health facilities, ambulatory surgery centers, medical office buildings, and senior living communities nationwide. The AI-augmented methodology evaluates physical infrastructure and operational processes against real-world threat scenarios — including active assailant, vehicle ramming, organized targeting, and opportunistic crime — and maps findings directly to security design improvements and, for eligible organizations, NSGP grant funding pathways.
Frequently Asked Questions
What is the most reliable physical security assessment method for hospitals?
No single method is sufficient. The most reliable approach combines on-site physical inspection with AI-augmented scenario modeling, operational process review, and clinical-area-specific evaluation. This layered methodology identifies how vulnerabilities across systems interact — something a standard walkthrough alone cannot capture.
How much does a physical security vulnerability assessment cost for a healthcare facility?
Costs vary based on facility size, number of buildings, clinical complexity, and scope. Some 501(c)(3) nonprofit healthcare organizations may offset costs through FEMA's Nonprofit Security Grant Program, which funds both assessment services and physical hardening improvements.
How often should healthcare organizations conduct physical security vulnerability assessments?
The Joint Commission requires annual worksite analysis related to workplace violence prevention. Beyond that minimum, assessments should be triggered by significant facility changes, mergers or acquisitions, new high-risk service lines (such as behavioral health expansion), or following a security incident. High-risk areas — emergency departments, behavioral health units — warrant more frequent review.
What is the difference between a vulnerability assessment and a penetration test in physical security?
A physical vulnerability assessment identifies and prioritizes weaknesses across the physical environment. A physical penetration test actively attempts to exploit those weaknesses — for example, testing whether a tailgating attempt succeeds or whether alarm systems respond as designed. Both serve distinct purposes and are increasingly expected under comprehensive security programs.
What regulations require healthcare organizations to conduct physical security assessments?
The Joint Commission EC.02.01.01 requires annual worksite analysis tied to workplace violence prevention. CMS Conditions of Participation (42 CFR 482.41) require maintenance of a safe physical environment. Several states — including California, Washington, Texas, and New York — have enacted binding workplace violence prevention laws with formal security assessment components.
Does physical security compliance overlap with HIPAA requirements?
HIPAA includes physical safeguard requirements under the Security Rule — covering workstation access, device controls, and facility access management. A physical security vulnerability assessment addresses the environmental controls side of these requirements, while cybersecurity assessments address electronic safeguards separately.