
Introduction
Hospitals are among the most complex environments to secure. Open 24 hours a day, flooded with foot traffic, and charged with emotionally volatile situations, they face threats most commercial security frameworks aren't built to handle: workplace violence, controlled substance theft, unauthorized access, and active assailant scenarios — often at the same time.
According to the Bureau of Labor Statistics, healthcare and social assistance workers experience workplace violence at a rate of 14.2 cases per 10,000 full-time workers — nearly five times the 2.9 per 10,000 rate for private industry overall.
A hospital security assessment is the structured process that moves a facility from guessing where it's vulnerable to knowing — and building a defensible plan to address it.
This article covers what a hospital security assessment involves, the four-step methodology behind it, what gets evaluated, and where assessments most commonly fall short.
Key Takeaways
- A hospital security assessment is a facility-wide review of physical security, operational processes, and regulatory compliance covering infrastructure, policies, staff, and compliance in one integrated process
- Regulatory requirements from HIPAA, OSHA, the Joint Commission, DEA, and state law (including California HSC 1257.7) make these assessments a legal requirement — not a discretionary best practice
- The process follows four steps: define objectives → identify threats and vulnerabilities → propose mitigation measures → implement solutions
- Key domains include physical infrastructure, emergency preparedness, policies and procedures, staff training, and controlled substance security
- Skipping or compressing steps leads to misallocated resources and security gaps — engage cross-functional teams and outside consultants to improve rigor
What Is a Hospital Security Assessment?
A hospital security assessment is a systematic, multi-domain evaluation of how effectively a facility can prevent, detect, and respond to physical threats. It is not a single inspection, not a compliance checklist, and not the same as ongoing monitoring.
Each serves a distinct purpose:
| Type | What it does |
|---|---|
| Security assessment | Proactive; identifies vulnerabilities and rates threats across all domains |
| Security audit | Evaluates compliance against a defined standard or checklist |
| Ongoing monitoring | Reactive; responds to incidents as they occur |
An assessment produces a documented understanding of current vulnerabilities, threat probabilities, and prioritized recommendations administrators can act on. It is typically conducted annually, following a significant incident, or after operational changes like facility renovations or leadership transitions.
The scope is broader than most administrators expect. A rigorous assessment covers:
- Physical infrastructure — access control, perimeter, surveillance, and weapons detection
- Operational processes — visitor management, lockdown procedures, and staff training
- Human-factor risks — modeled against active assailant events, organized targeting, and opportunistic crime
Why Hospital Security Assessments Are Non-Negotiable
Healthcare and social assistance accounted for 72.8% of all nonfatal workplace violence cases in private industry in 2021–2022, per BLS data. The financial exposure compounds that risk: the IBM Cost of a Data Breach Report 2025 puts the average cost of a healthcare breach at $7.42 million — the highest of any sector.
Physical violence and data exposure aren't the only threats. Per ASHP, controlled substance diversion creates patient safety risks, legal liability, and reputational harm — compounded by DEA enforcement when controls fail.
Regulatory Drivers
Formal assessments aren't just good practice — they're legally required across multiple frameworks:
- HIPAA (45 CFR 164.308): mandates accurate risk assessments of threats to electronic protected health information
- OSHA General Duty Clause: requires a workplace free from recognized hazards; workplace violence planning is an active enforcement priority in healthcare
- Joint Commission (EC.02.01.01): requires annual security management plan evaluations; defines "secure" as locked, surveilled, or under constant supervision
- DEA (21 CFR Part 1301): requires access controls against diversion and theft reporting within one business day
- CMS (42 CFR 482.15): requires emergency preparedness programs grounded in documented facility and community risk assessments, reviewed every two years
- California HSC 1257.7: mandates annual assessments covering violent behavior trends, facility layout, staffing, and training

Violations across these frameworks carry financial penalties, accreditation consequences, and in some cases criminal liability — which is why a structured four-step assessment process matters.
The Four Steps of a Hospital Security Assessment
The components evaluated in a hospital security assessment vary by facility, but the process follows a consistent four-step sequence. Each step informs the next — teams that skip ahead to implementation without rigorous threat identification risk spending on the wrong interventions.
Step 1: Define Assessment Objectives
Before any assessment begins, security personnel and management should review previous incident logs, near-miss reports, and local crime data to identify patterns. This intelligence determines which domains — physical safety, controlled substances, emergency response, access control — require the most scrutiny.
Clear objectives make the assessment actionable. A hospital with a recent ER violence incident has different priorities than one that experienced unauthorized pharmacy access. Without defined scope, the assessment becomes generic and produces recommendations that don't reflect the facility's actual risk profile.
Step 2: Identify Threats and Vulnerabilities
This phase maps out every credible threat — acts of aggression, active assailant scenarios, medication theft, vandalism, vehicle ramming, and natural disasters — and rates each by likelihood and potential impact based on the facility's layout, occupancy patterns, and incident history.
Vulnerability identification must extend well beyond obvious entry points:
- Internal risks: disgruntled employees, lapses in controlled substance handling, tailgating through secure doors
- Environmental gaps: parking lot blind spots, unmonitored service entrances, inadequate lighting near perimeter access points
- Operational weaknesses: inconsistent visitor credentialing, unclear after-hours access protocols, untested lockdown procedures
- Physical infrastructure: surveillance dead zones, alarm systems that don't communicate with access control, unprotected infant and pediatric units
The output of this phase is a threat register — a documented inventory of risks, ranked by severity, that feeds directly into the next step.
Step 3: Propose Risk Mitigation Measures
With threats ranked, the team builds a prioritized action plan. Finite budget should flow toward highest-risk vulnerabilities first, not be spread evenly across every finding.
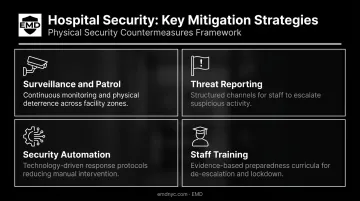
Mitigation typically falls into four categories:
- Surveillance and patrol — close coverage gaps, update patrol routes based on identified blind spots
- Threat reporting — give staff accessible channels to flag suspicious activity and near-misses before incidents escalate
- Security automation — integrate alarm triggers, lockdown systems, and access control so each component activates the others
- Staff training — build competency in de-escalation, emergency response, and tailgating prevention at every level
This is also the stage where working with a specialized physical security consultancy adds the most value. A firm like EMD analyzes how vulnerabilities intersect across systems — access control gaps that compound surveillance blind spots, for example — rather than treating each finding in isolation. EMD can also map mitigation recommendations to available grant funding, including NSGP for eligible nonprofit healthcare organizations, to reduce out-of-pocket implementation costs.
Step 4: Implement New Security Solutions
With a prioritized mitigation plan in hand, implementation can begin — and it involves more than installing hardware. Systems must be configured to communicate: access control triggering cameras and alarms, lockdown protocols tied to notification systems. Organizational policies, staff training curricula, and assessment documentation all require updating to reflect the new security posture and support regulatory compliance.
Teams should work through key questions across each security domain during implementation:
- General security: Incident reporting procedures documented and current?
- Video surveillance: Coverage confirmed across ED waiting rooms, pharmacy, and infant/pediatric units?
- Access control: Credential issuance and revocation enforced consistently?
- Emergency systems: Lockdown procedures tested, with staff clear on their roles?
- Security personnel: Staffing levels and post assignments aligned with assessed risk?
Key Components Evaluated During a Hospital Security Assessment
Physical Security
Assessors review both the physical condition and operational configuration of:
- Access control systems at all entry points, including after-hours access
- Video surveillance placement, coverage angles, and recording retention
- Perimeter security — fencing, bollards, lighting, and controlled parking access
- Alarm and intrusion detection systems, including sensor placement
- Weapons detection tools and deployment protocols
- Emergency infrastructure: lockdown capabilities, shelter-in-place systems, evacuation routes
Healthcare-specific areas requiring dedicated attention include emergency department access, behavioral health unit safety, infant and pediatric protection zones, helipad security, and medication storage.
Policies and Procedures
Technically sound security systems fail when policies are outdated or inconsistently applied. Assessors review:
- Credential issuance and revocation procedures
- Controlled substance handling protocols
- Visitor management processes
- Incident reporting standards
- Documented emergency response plans for active shooter events, fires, and mass casualty situations
Employee Training
Staff behavior is where well-designed security systems most often break down in practice. The Joint Commission requires training at hire, annually, and when program changes occur — covering workplace violence definitions, de-escalation, emergency response, and incident reporting.
An effective assessment evaluates training depth, not just existence. Key indicators include:
- Whether staff can demonstrate competency, not just confirm they attended training
- How recently the facility conducted a live active shooter or lockdown drill
- Whether de-escalation protocols are practiced regularly or only documented
Regulatory Compliance Verification
The assessment must confirm alignment across:
- HIPAA Privacy and Security Rules (with cybersecurity components referred to a qualified IT security partner)
- OSHA workplace safety standards
- DEA controlled substance storage and reporting requirements
- CMS emergency preparedness conditions of participation
- Joint Commission environment-of-care standards
Note: EMD's assessments cover the physical and operational dimensions of compliance across these frameworks. HIPAA cybersecurity and IT security architecture fall outside this scope and should be addressed by a qualified cybersecurity firm.
Common Gaps in Hospital Security Assessments
Treating It as a One-Time Event
Threats evolve. New staff, facility renovations, changes in local crime patterns, software updates, and regulatory shifts all alter a hospital's security profile. Assessments should be conducted at minimum annually — and following any significant incident or operational change. The Joint Commission explicitly identifies annual evaluation of security management plans as a requirement.
Siloing Physical and Cybersecurity
Hospitals frequently run IT security and physical security assessments through separate organizational workstreams. This creates blind spots. An unsecured server room is a physical security failure. A compromised access control system is a hybrid security risk. CISA's guidance on converged security notes that integrated cyber-physical functions help organizations identify and respond to hybrid attacks that neither team would catch independently.
Underinvesting in Training Evaluation
Assessment resources tend to concentrate on technology and infrastructure — training gets treated as a checkbox. That's a problem. Untrained staff create exploitable vulnerabilities that no camera or lock can fully compensate for.
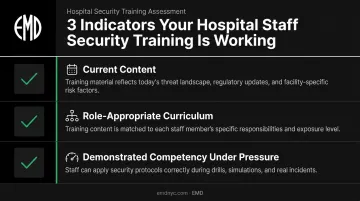
The training evaluation component should confirm:
- Whether training content is current and reflects recent threat scenarios
- Whether the curriculum covers the right situations for each staff role
- Whether employees can demonstrate competency under realistic pressure
Frequently Asked Questions
How often should a hospital conduct a security assessment?
Most regulatory frameworks and industry standards recommend annual assessments at minimum. Additional assessments should be triggered by significant incidents, facility renovations, major regulatory updates, or leadership transitions that affect security decision-making.
What regulations require hospitals to conduct security assessments?
Primary drivers include HIPAA (45 CFR 164.308), OSHA's General Duty Clause, Joint Commission environment-of-care standards, DEA regulations under 21 CFR Part 1301, CMS emergency preparedness requirements under 42 CFR 482.15, and state mandates such as California's annual requirement under Health and Safety Code 1257.7.
Who should be involved in a hospital security assessment?
Effective assessments require cross-functional participation: hospital administrators, facilities management, clinical department heads, HR, and frontline staff. External physical security consultants are often engaged to provide objectivity, specialized methodology, and familiarity with applicable grant funding programs.
What is the difference between a hospital security assessment and a security audit?
A security audit evaluates compliance against a defined standard or checklist. A security assessment is a broader, proactive investigation that identifies vulnerabilities, rates threats by likelihood and impact, and generates tailored recommendations. Both tools serve distinct purposes and work best when used together.
How long does a hospital security assessment typically take?
For a mid-size hospital, a thorough assessment generally spans several weeks — covering on-site walkthroughs, document review, stakeholder interviews, vulnerability analysis, and producing a written findings report with prioritized recommendations.
Can hospitals access grants or funding to implement security improvements?
Federal and state funding programs exist to help qualifying institutions finance security upgrades. Nonprofit healthcare organizations may be eligible for FEMA's Nonprofit Security Grant Program (NSGP). A physical security consultancy experienced in grant management, such as EMD, can help administrators identify eligible programs and navigate the application process.


