Those numbers aren't just a workforce safety problem. Violence exposure drives staff burnout, feeds turnover, and directly compromises patient care. A 2024 JAMA Network Open meta-analysis of 85 studies and 288,581 nurses linked nurse burnout to more medication errors, more falls, more infections, and lower patient satisfaction scores. The violence-to-burnout-to-patient-harm chain is well-documented and getting harder to ignore.
This guide covers the organizational, cultural, and physical security strategies that, together, form a defensible prevention framework — because no single intervention fixes this problem alone.
Key Takeaways
- Healthcare workers make up nearly three-quarters of all private-industry workplace violence injuries
- Violence spans verbal threats, intimidation, patient/family assaults, and coworker bullying — all cause measurable harm
- Prevention requires policy, staff training, reporting systems, and physical security — working in layers
- Most incidents go unreported due to fear, normalization, and broken reporting processes
- This is an institutional responsibility, not something individual staff can solve on their own
Understanding Workplace Violence in Healthcare Settings
Who Gets Hurt and Where
The Joint Commission defines workplace violence broadly: "an act or threat occurring at the workplace" that includes "verbal, nonverbal, written, or physical aggression; threatening, intimidating, harassing, or humiliating words or actions; bullying; sabotage; sexual harassment; physical assaults; or other behaviors of concern involving staff, licensed practitioners, patients, or visitors."
That definition matters because organizations tend to focus on physical assaults while ignoring the verbal and psychological violence that happens constantly. NIOSH-cited population data puts physical assaults at 13.2 per 100 nurses per year — but nonphysical violent events at 38.8 per 100 nurses per year. The verbal incidents cause real harm even when they leave no visible injury.
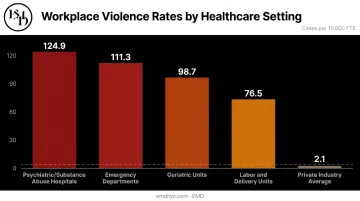
High-risk settings aren't limited to one unit type. BLS data identifies psychiatric and substance abuse hospitals at 124.9 cases per 10,000 FTE — the highest rate by far. Emergency departments, waiting rooms, geriatric units, and labor and delivery units all appear consistently in the research as elevated-risk environments.
Why Healthcare Is Structurally Vulnerable
Several factors converge to make healthcare uniquely dangerous:
- Emotional volatility — patients and families are often frightened, in pain, or receiving catastrophic news
- Long wait times without communication, which escalates anxiety and frustration
- Overnight and weekend shifts reduce supervisory presence and limit controlled access
- Staff shortages and overcrowding stretch incident response capacity thin
- Public movement goes largely unrestricted in many facilities, especially those built before controlled-access standards were common
- Substance use and cognitive impairment in patient populations increase unpredictability
These clinical risk factors compound systemic vulnerabilities. A psychiatric unit with inadequate staffing and poor sightlines doesn't just face elevated risk — it faces risk that goes unmitigated until something goes wrong. That's what makes the underreporting problem so consequential.
The Underreporting Problem
Most violence incidents in healthcare go undocumented. A 2024 Journal of Clinical Nursing analysis found reporting rates in studied populations ranged from 6.5% to 30%, with ANA estimates ranging from 20% to 60%. The three most common reasons nurses gave for not reporting:
- 60.8% to 74.6% believed nothing would change
- 45.5% experiencing coworker violence cited fear of retaliation
- 32.2% didn't know the formal reporting process
This gap is an organizational failure. When data doesn't get captured, patterns go undetected, resources get misallocated, and the underlying conditions that enable violence remain unaddressed.
Prevention Guidelines for Healthcare Settings
Effective prevention operates at three levels simultaneously: institutional policy, staff preparedness, and physical security design. A gap at any level undermines the others.
Building Organizational Policies and Accountability
A formal written workplace violence prevention program is the foundation. At minimum, it should define the scope of covered behaviors, assign clear leadership accountability, establish incident response protocols, and align with OSHA's Guidelines for Preventing Workplace Violence for Healthcare and Social Service Workers.
Since January 1, 2022, The Joint Commission has required accredited hospitals to manage and investigate workplace violence risks as part of accreditation standards. Specific standards cover leadership oversight (LD.03.01.01 EP 9), annual worksite analysis (EC.02.01.01 EP 17), and staff education at hire and annually (HR.01.05.03 EP 29). Facilities that aren't benchmarking against these standards are already behind.
Beyond policy documents, organizations need functioning reporting systems. The data on why staff don't report points directly to what needs to change:
- Reporting tools that are complicated or time-consuming create friction that kills compliance
- Fear of retaliation means non-punitive policies must be explicit and consistently enforced
- Belief that "nothing will be done" means leadership must visibly act on reports, conduct post-incident debriefs, and communicate outcomes back to staff
Leadership tone matters more than the policy document itself. When management is seen as dismissive of violence reports, every other prevention measure loses credibility.
Staff Training and De-escalation
All healthcare staff — not just security personnel — need foundational training in recognizing escalation cues, applying de-escalation techniques, and following facility response protocols.
Research consistently shows that training improves confidence and knowledge, but it does not reliably reduce violence rates when deployed as a standalone intervention. It fills a gap; it doesn't substitute for structural change.
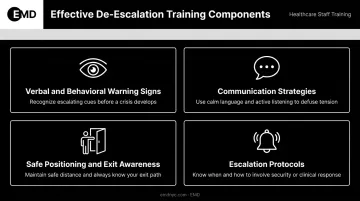
Effective de-escalation training should cover:
- Verbal and behavioral warning signs — raised voice, agitated pacing, refusal to cooperate, verbal threats
- Communication strategies — tone, pacing, language that reduces tension rather than escalates it
- Safe positioning and exit awareness — spatial awareness during high-risk interactions
- Escalation protocols — when to call for backup rather than attempting independent intervention
Training must be recurring. A one-time onboarding module doesn't sustain skills or keep pace with changes in patient population or facility environment. Post-incident support — including access to mental health counseling — is equally non-negotiable. Staff who experience violence and receive no support don't just leave; they become unsafe at work before they do.
Physical Security and Environmental Design
Training addresses how staff respond. Environmental design determines the conditions they're responding in — and it remains one of the most underused tools in healthcare violence prevention. Layout decisions, lighting, access control, and sightlines can either create or eliminate the conditions where violence occurs.
Key engineering and access controls to evaluate:
- Controlled entry points at emergency department and behavioral health unit access
- Visitor management systems with identity verification
- Panic buttons and duress alarms at high-exposure locations (triage, reception, exam rooms)
- CCTV placement covering waiting rooms, corridors, and parking areas with appropriate monitoring
- Clear sightlines from nursing stations to patient areas
- Physical barriers at reception — desk shields, deep service counters, or bullet-resistant glazing in high-acuity units
Physical separation also matters: separate waiting areas for agitated patients reduce escalation opportunities, and secure medication storage eliminates a common trigger for drug-seeking violence.
Security staffing decisions don't operate independently of design. A well-trained security team working in a poorly laid-out facility — no clear sightlines, no fast response corridors, inadequate communication infrastructure — will consistently underperform. Physical design and personnel protocols need to be developed together.
An external security assessment surfaces vulnerabilities that internal staff, through familiarity alone, often miss. EMD provides AI-augmented physical security vulnerability assessments for healthcare facilities — covering emergency department access, behavioral health unit safety, visitor management, after-hours access, and multi-building campus design — evaluated against Joint Commission environment-of-care standards.
Recognizing Warning Signs Before Violence Escalates
Most physical violence incidents are preceded by observable signals. Staff who recognize these early have a window for intervention. Those who miss them often find themselves reacting instead of responding.
Patient-specific and situational risk indicators:
- Known history of aggression documented in the patient record
- Substance use, intoxication, or withdrawal
- Cognitive impairment or altered mental status
- Prolonged wait time without staff communication
- Family members under acute distress
- Overcrowded or high-noise environments
Structural practices that reduce surprise:
- Flag known behavioral risk in scheduling and handoff communications
- Use structured safety huddles before high-risk interactions
- Document behavioral flags in clinical records so the next clinician isn't starting blind
The goal isn't to profile patients — it's to approach high-risk interactions with preparation. When behavioral history is documented and communicated, staff can adjust their positioning, modify their communication style, and have support standing by before a situation escalates. Preparation is what separates a managed interaction from an incident report.
Common Prevention Mistakes to Avoid
Normalizing Violence as "Part of the Job"
This attitude — widespread among experienced healthcare staff — is one of the most damaging barriers to prevention. It suppresses reporting, delays institutional response, and allows risk factors to build undetected. NIOSH explicitly identifies normalization and victim-blaming as primary reporting barriers, and the 2024 data confirms that the majority of non-reporters simply didn't believe anything would change.
The organizational consequence is data blindness. When incidents go unreported, patterns don't emerge, high-risk units don't get flagged, and resource allocation stays misaligned with actual need.
Relying on Training Without Fixing the Environment
Training-only programs are the most common prevention mistake healthcare organizations make. They're deployable, documentable, and feel like action — but systematic reviews consistently show they improve knowledge and confidence without reliably reducing incident rates when not paired with structural supports.
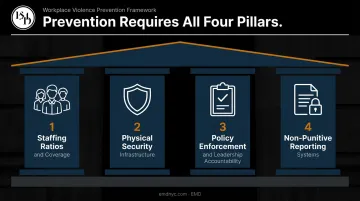
Effective prevention requires simultaneous action on:
- Staffing ratios and coverage gaps
- Physical security infrastructure
- Policy enforcement with visible leadership accountability
- Accessible, non-punitive reporting systems
Training addresses a real knowledge gap. Without structural fixes alongside it, incident rates don't move.
Treating Prevention as a One-Time Initiative
Facilities that complete a security assessment or roll out a training program and consider the problem "addressed" are exposed to compounding risk. Violence risk shifts with patient populations, staffing levels, facility renovations, and seasonal demand — none of which pause after a program launch.
Sustained prevention requires:
- Continuous incident monitoring and trend analysis
- Periodic reassessment tied to operational changes
- Leadership accountability that outlasts the initial rollout
Frequently Asked Questions
How can we prevent workplace violence in healthcare?
Prevention requires a layered approach: formal organizational policies, staff training in recognition and de-escalation, accessible non-punitive reporting systems, and physical security controls working together. No single intervention is effective in isolation — the evidence consistently favors multicomponent programs.
What are the most common types of workplace violence in healthcare settings?
Patient and family-to-staff violence is the most prevalent type, but coworker-to-coworker horizontal violence and bullying are also widespread, with some studies reporting rates above 50% in certain units. Verbal violence is the most frequent form overall, occurring at rates nearly three times higher than physical assault, and is the most underreported.
Why is workplace violence so underreported in healthcare?
The three primary barriers are fear of retaliation, the belief that nothing will be done, and normalization of violence as an expected occupational hazard. Cumbersome reporting tools add further friction, which means the actual scope of the problem is consistently larger than incident data suggests.
What training is most effective for healthcare staff?
Training in early warning sign recognition, de-escalation, and response protocols builds staff confidence. It must be paired with organizational and environmental supports — staffing, physical security, reporting culture — to produce reliable reductions in incident rates.
How does physical security design help prevent workplace violence?
Controlled entry points, duress alarms, strategic camera placement, clear sightlines, and physical barriers like reception shields reduce both the opportunity and severity of violent incidents. A formal security assessment can identify facility-specific vulnerabilities that generic checklists miss.
How does workplace violence in healthcare affect patient safety?
Violence-exposed staff experience burnout, distraction, and PTSD, all of which increase medication errors, reduce care quality, and accelerate turnover. Research establishes a direct chain from workforce safety to patient outcomes: organizations that ignore staff violence exposure accept worse patient safety performance as a result.